Good news for weekend warriors: Rehab is shown to prevent knee surgery.* This may seem like a no brainer to some, but common orthopedic wisdom is that ACL tears–a common type of knee injury in athletes–almost always require surgery. New research shows, however, that rehab-first may be a better option.
A study of Swedish amateur athletes–mostly soccer players–found that those who got anterior cruciate ligament (ACL) surgery right away plus physical therapy fared no better than those that got the knee rehab first; and although 50% of the rehab-first subjects eventually required surgery, they were not any worse off than had they gotten the surgery early on.
The implications of this study are that people suffering from ACL tears can and should try rehab before going under the knife. If it isn’t obvious, all surgery has inherent risk due to the invasive nature of the procedure. Also, at $10K+ per pop (no pun intended), these results are economically encouraging. If you end up needing surgery later, you can still get it with little fear of turning out worse for waiting.
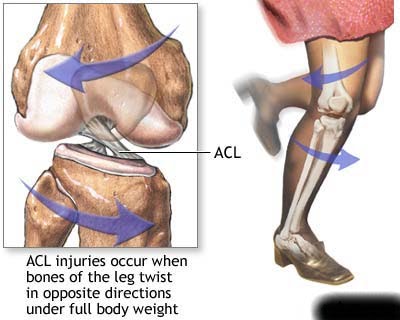 The anterior cruciate ligament (ACL) is one of four major ligament of the knee. Its function is to prevent forward, or anterior, movement of the tibia (shin bone) on the femur (thigh bone). It is the most commonly injured ligament in the knee. Football, soccer and basketball players are particularly prone to ACL tears, as are skiers, as a result of the pivot and twist motions required in these sports.
The anterior cruciate ligament (ACL) is one of four major ligament of the knee. Its function is to prevent forward, or anterior, movement of the tibia (shin bone) on the femur (thigh bone). It is the most commonly injured ligament in the knee. Football, soccer and basketball players are particularly prone to ACL tears, as are skiers, as a result of the pivot and twist motions required in these sports.

Approximately 200,000 Americans go through ACL reconstruction each year, although many people can get by with a knee brace and rehab. But, of course, getting the surgery depends on how the injury affects one’s lifestyle.
The study’s results showed that both the surgery-first and rehab-first groups fared about the same when it came to things like pain, performance in sports and how much their knee interfered with their lives. Of those that received rehab first, about 40% needed to get the surgery later, and this group fared no better or worse than those that didn’t get the surgery at all.
 One problem with the study is that the results were only measured after two years, so there could be some changes later. The researchers will be doing a follow up at five years to study outcomes at that time. Also, it appears that the rehabilitation group showed some signs of trouble with the meniscus, a cushioning disk in the knee joint, which some doctors think could increase the risks of degenerative arthritis in the future.
One problem with the study is that the results were only measured after two years, so there could be some changes later. The researchers will be doing a follow up at five years to study outcomes at that time. Also, it appears that the rehabilitation group showed some signs of trouble with the meniscus, a cushioning disk in the knee joint, which some doctors think could increase the risks of degenerative arthritis in the future.
I find this study interesting and the results encouraging, because I was also under the impression that ACL tears pretty much required surgery. Being a Los Angeles sports chiropractor, I see my fair share of knee injuries, and torn ACLs definitely limp into my office from time to time. But now I’ll be a little less quick to refer the client out to an orthopedist. Six months of rehab might be just fine in some of those cases. Thank you, Swedes, for the great work!
*A Randomized Trial of Treatment for Acute Anterior Cruciate Ligament Tears