
I recently posted on some telling “health” statistics in the U.S. It’s so refreshing to know what Americans are really fighting for with regard to health care, because the strong belief of some is that every American has the right to be on as many drugs as their neighbor. For the mass American mentality–that’s health! Awesome.
Americans are fighting for their inalienable right to drug their children. Yes, they are…that’s health, remember? If parents can’t understand their children, and public school officials can’t understand their children, then their good doctors will be there to help. Yes…with anti-depressants. In fact, more children are on psychoactive drugs today than on any other drug ever before in history.
 Is it me? Do I just not understand health or health care? Are we blessed–part of the “haves”–if we can get antidepressants for our children? Ohhhhh…maybe I’d better go back to doctor school. I thought health and wellness was something else.
Is it me? Do I just not understand health or health care? Are we blessed–part of the “haves”–if we can get antidepressants for our children? Ohhhhh…maybe I’d better go back to doctor school. I thought health and wellness was something else.
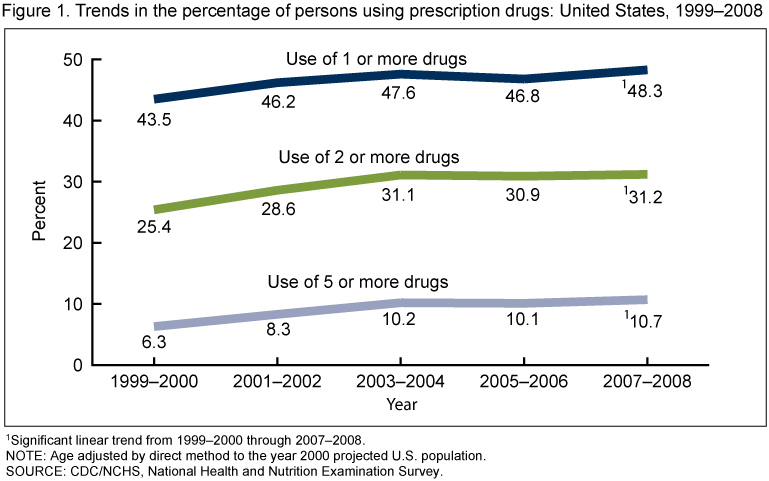
According to the CDC’s National Center for Health Statistics study published in September 2011, antidepressants were the third most common prescriptiondrugtaken by Americans of all ages in 2005–2008.
And from 1988-1994 through 2005-2008, the rate of antidepressant use in the United States among all ages increased nearly 400%.
Isn’t that awesome? Aren’t we so fortunate here in the U.S.? Hope Obamacare brings antidepressant drugging to every citizen in the nation, especially children. It’s our right to NOT be sad. Yay, Obamacare!!!
Here go some more stats for you:

- 11% of Americans aged 12 years and over take antidepressant medication.
- Females are more likely to take antidepressants than are males, and non-Hispanic white persons are more likely to take antidepressants than are non-Hispanic black and Mexican-American persons.
- About one-third of persons with severe depressive symptoms take antidepressant medication.
- More than 60% of Americans taking antidepressant medication have taken it for 2 years or longer, with 14% having taken the medication for 10 years or more.
- Less than one-third of Americans taking one antidepressant medication and less than one-half of those taking multiple antidepressants have seen a mental health professional in the past year.
I love these statistics. They show how much healthier we are as a result of the mass antidepressant prescription campaign. Thank you Obamacare, for caring so much that you want me and my children to have as many antidepressants as we need. No more sadness for us. We are so fortunate to have real health care in this country; and so fortunate that we may all get even more courtesy of our federal government and caring medical industry. Truly awesome.






































{kind=link}