One of the biggest messages I try to put forth in this blog is that human beings are amazing self-healing, self-regulating life forms. We operate under the laws of the universe, and as such, by obeying some very fundamental principles regarding life, our ability to experience great physical health and well-being is magnified. It doesn’t matter whether you have any particular genetic, anatomic or physiologic disposition–you can experience great health, as well as a fulfilling life, by observing basic principles.
This is as true for the “normal” individual as it is for the ADD-labeled person. Whenever somebody comes to me with this or that problem, my first investigation as a doctor is to find out if they are observing the basics. So that’s what I want to finish off with regarding ADD. It’s of mega-importance that your ADD-labeled child is practicing the healthiest lifestyle possible. But take note, and do not mistake this very crucial point: What I discuss here is NOT a treatment regimen for ADD. I do NOT believe that an attention deficit is a disorder, therefore nothing needs treating, especially as we would think in a mechanistic sense. Instead, what I put forth here will allow any child to thrive physically and mentally, because these are fundamental health principles.
There are no absolutes when it comes to health. No one practice is more important than another–let’s just get that straight right from the beginning. Instead, health is like a puzzle, and each practice is a piece to that puzzle. I will for brevity’s sake only touch upon each puzzle piece. If you want more, then I highly recommend reading my book, The Six Keys to Optimal Health. In it you will find most of these points discussed in full detail, along with tips on how to best implement and maximize each practice.
First and foremost is diet and nutrition. It should go without saying that good nutrition is paramount to a healthy functioning body, but I wonder sometimes. Too many parents feed their children foods that are, well…suspect. Here is a basic: foods should be whole and natural. I’m not saying organic or hormone free or anything like that. If that’s what you prefer, awesome! But what I mean is “not processed”. Lots of fresh fruits and vegetables, fresh meats and dairy, wholesome grains, minimal sugar, minimal fast food (or none at all, like my kids), and definitely, with no exception: NO SODA!
Soda consumption should be the biggest no-no for an ADD-labeled child. No, I don’t think soda causes ADD. Soda is garbage for anybody, and that much sugar consistently cannot be conducive to mental sharpness. Sad fact is that many parents will have to kick their own liquid garbage habit, too, if they want to keep their kids off it.
 Next is exercise*. Kids need to spend time playing and moving! Period. It is a standard recommendation for ADD-labeled kids to exercise often, and I couldn’t agree more. Get your kids moving everyday–that’s what our bodies (and all life forms) are meant to do. Don’t try operating outside of universal laws and then also expect good health. *Check out this interesting article on children, exercise balls, and focus.
Next is exercise*. Kids need to spend time playing and moving! Period. It is a standard recommendation for ADD-labeled kids to exercise often, and I couldn’t agree more. Get your kids moving everyday–that’s what our bodies (and all life forms) are meant to do. Don’t try operating outside of universal laws and then also expect good health. *Check out this interesting article on children, exercise balls, and focus.
Next, bodywork. If you haven’t taken your ADD-labeled child to see a chiropractor, then you are doing them a great disservice. Subluxations (misaligned and stuck vertebrae) are extremely disruptive to the nervous system and the mind. I have seen hundreds of children go into a state of ease and calm following a chiropractic adjustment. Time to learn more about chiropractic and give it a try if your knowledge and experience are limited.
**Throughout these posts, a regular reader and friend, has been kind enough to share her understanding and insight of primitive movement patterns and neurological development. I am so fascinated and intrigued by this field of study that I intend to investigate it further. She swears by its benefits, and I respect her knowledge and judgment. I will keep you informed as I learn more. Thank you K.O.

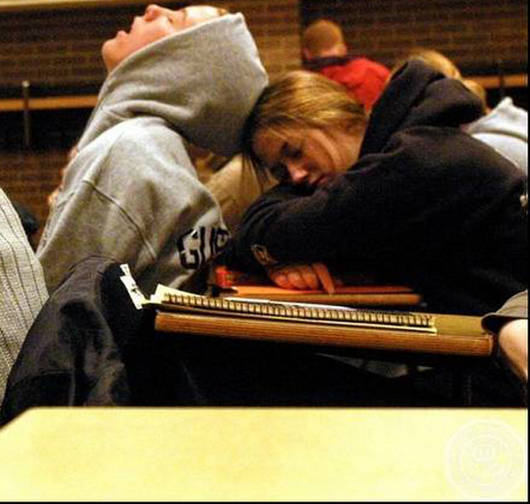
Sleep is next. But we could just as well call this rest and recuperation. If your child is not sleeping properly, then they are aging faster and breaking down more quickly. Sleep is essential to life. Many metabolic and regenerative processes occur while we sleep.
And don’t discount dreaming. Although we still understand little about this ubiquitous function, I believe it has an important role in our mental brain states (no, I do not think dreams are symbolic).
If your ADD-labeled child is on Ritalin, then I would expect his or her sleep to be disrupted, particularly deep and REM sleep. Think about that–it’s just another way that these dangerous drugs can hurt your child. If they are also hopped-up on soda…(sigh) heaven help them.
Next is minimizing toxins. Lot’s of things are toxins, but the ones I find most prevalent and damaging are…drum roll please…prescription and over-the-counter drugs. Nothing wrong these meds periodically when needed, but as a society, Americans are way too over-medicated. Just look at the Ritalin numbers: 90% consumed in the U.S. Sad.

Finally is the mental health. When it comes to your ADD-labeled child, they want what every child (and every person, for that matter) wants–love and acceptance for who they are. So, again, help them find what they love–they know what it is, because they do it all the time.
Be it sports, be it music, be it socializing, be it fashion–find it, nurture it, and help them be inspired by it. Pressuring your kid–directly or passively–is not going to help. When a child senses that you are worried, frustrated, or disappointed, they know it; and trust me this only will add to their stress and inability to perform. Let them know you love, honor and support them in whatever they love doing, and they will reward you by excelling. No, they may never excel in school, but plenty of people live amazing lives that were not the result of traditional schooling.
There you have it–like pieces to a puzzle. Each one important, but neither more-so than any of the others. In fact, they work synergistically, but I’ll leave that topic for you to read in my book.
Once again, I sincerely hope I’ve helped people facing some tough decisions regarding their own ADD-labeled child. If I can have helped you see your beautifully unique and gifted genius in a new light, then I am pleased. If I’ve influenced you to reject the dangerous chemical poisons that the ADD establishment wants to numb your child on, then I am honored. If I’ve given you some ideas on how to inspire your child to be all that they can be, then I am utterly grateful that I could contribute.
Thank you for reading.